
From Blood Pressure to Tranexamic Acid—Rethinking the Science of Bleeding Control in Oral Surgery
The most important instrument in oral surgery is not the forceps. It is judgment.
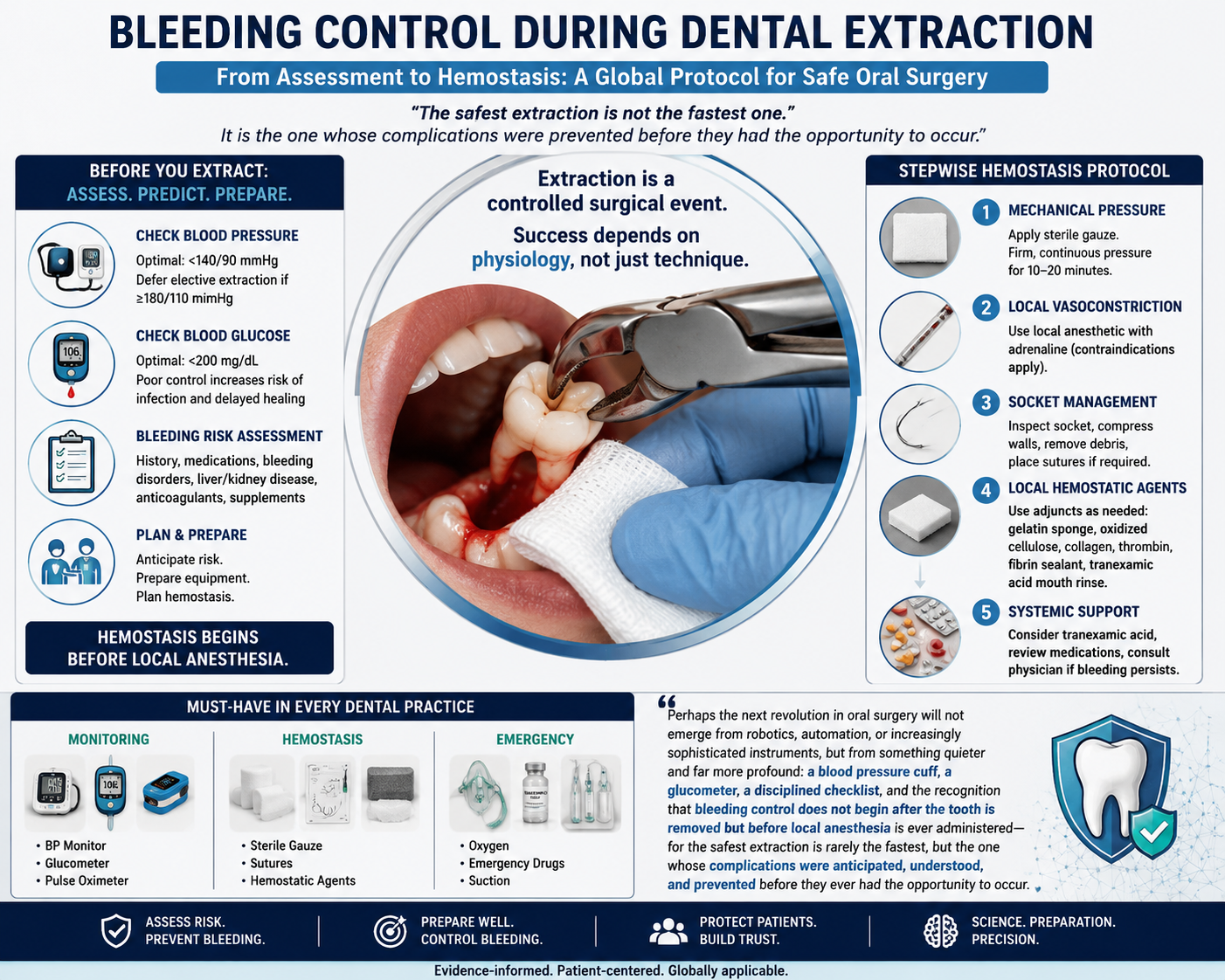
Dental extraction is frequently described as one of the most routine procedures in healthcare. Yet the word routine often disguises an important truth: extraction is a controlled vascular injury.
Most extraction-related bleeding is not unexpected. It is predictable.
And what is predictable should be preventable.
Modern oral surgery increasingly recognizes that successful hemostasis begins before tissue is touched. In an era of digital dentistry, guided surgery and artificial intelligence, there remains a surprisingly under-discussed question:
Why do many dental clinics still measure neither blood pressure nor blood glucose before performing invasive treatment?
This blog proposes that global dentistry should move from a tooth-centred extraction model to a physiology-centred extraction protocol.
Extraction Is Not a Tooth Procedure. It Is a Surgical Event.
Every extraction disrupts:
- arterial inflow,
- venous drainage,
- capillary integrity,
- platelet recruitment,
- coagulation pathways,
- fibrin formation,
- tissue healing.
Whether bleeding remains controlled depends on the interaction between:
Patient × Procedure × Pharmacology × Preparedness
A healthy young adult undergoing removal of a mobile deciduous tooth is biologically different from:
- a hypertensive executive,
- a diabetic patient,
- an anticoagulated elderly patient,
- a patient with occult platelet dysfunction,
- a patient with liver disease,
- a patient who has never previously undergone surgery.
The socket is not aware of how experienced the surgeon is.
The socket responds only to biology.
Phase I — Predict Before You Extract
1. Vital Signs Are Not Optional
Chairside physiological assessment should become normalised globally.
Blood Pressure
Preoperative blood pressure assessment is arguably the most underutilised risk-reduction strategy in routine dentistry.
Elevated blood pressure:
- increases capillary hydrostatic pressure,
- complicates local vasoconstrictor selection,
- may increase postoperative ooze,
- may signal broader cardiovascular instability.
Suggested practical framework (institution-dependent):
| Blood Pressure | Suggested Action |
|---|---|
| <140/90 | Proceed |
| 140–159 / 90–99 | Proceed cautiously |
| ≥180 systolic or ≥110 diastolic | Defer elective extraction |
Importantly:
Hypertension is not a coagulation disorder.
But pressure challenges clot stability.
2. Blood Glucose: A Hemostasis Marker Hidden in Plain Sight
Blood glucose screening is often viewed only through the lens of diabetes.
That is incomplete.
Poor glycaemic control affects:
- platelet interaction,
- endothelial response,
- inflammation,
- healing kinetics,
- infection susceptibility.
Extraction success should not be measured at one hour.
It should be measured at seven days.
Routine chairside glucose evaluation may identify patients whose healing trajectory is already compromised.
3. Bleeding Risk Assessment Must Evolve Beyond Tradition
Historically, bleeding time was widely used.
Modern evidence supports more targeted approaches.
A practical hierarchy:
First-line
- structured bleeding history,
- medication review.
Second-line (when indicated)
- platelet count,
- PT,
- INR,
- aPTT.
Advanced evaluation
- platelet function studies,
- specialist consultation.
One carefully asked question often prevents more bleeding than one additional hemostatic material.
Phase II — The Sequential Science of Hemostasis
Hemostasis during extraction follows physiology.
Not panic.
Step 1 — Mechanical Compression
First intervention.
Always :
- Place sterile gauze.
- Maintain uninterrupted compression:10–20 minutes minimum.
- Repeated inspection destabilises clot formation.
- The clot must mature before it is judged.
Step 2 — Pharmacological Vasoconstriction
Local anesthetic containing adrenaline (epinephrine), where medically appropriate, remains among the most elegant tools in oral surgery.
Mechanisms:
- arteriolar constriction,
- reduced local perfusion,
- improved visualisation,
- enhanced operative precision.
Clinical judgment remains essential in patients with selected cardiovascular conditions.
Adrenaline should not replace surgical skill.
It should amplify it.
Step 3 — Tissue Stabilisation
If bleeding continues:
- inspect socket walls,
- compress bone,
- remove granulation tissue where appropriate,
- identify vessel injury,
- suture.
Sutures should be viewed not merely as wound closure.
They are mechanical hemostatic devices.
Step 4 — Local Hemostatic Architecture
Every extraction clinic should maintain immediate access to local hemostatic adjuncts.
Recommended Core Inventory
Absorbable Materials
- gelatin sponge,
- oxidised regenerated cellulose,
- collagen matrix.
Biological Agents
- topical thrombin,
- fibrin sealants.
Antifibrinolytics
- tranexamic acid mouth rinse.
Hemostatic materials should support clot formation.
They should never substitute diagnosis.
Step 5 — Systemic Support
Persistent bleeding may require escalation.
Potential approaches include:
- oral tranexamic acid,
- intravenous antifibrinolytics,
- anticoagulant modification (physician-guided),
- factor replacement,
- platelet support.
Escalation should follow protocol.
Not improvisation.
The Extraction Emergency Cart: A Global Minimum Standard
If a practice removes teeth, it should be equipped to stop bleeding.
Monitoring
✓ Blood pressure monitor
✓ Pulse oximeter
✓ Glucometer
Hemostasis
✓ Sterile gauze
✓ Suture kit
✓ Local hemostatic agents
Emergency Support
✓ Oxygen
✓ Suction
✓ Emergency medications
The economics are simple.
“A delayed emergency referral costs more than preparation.”
A Proposal for Global Dentistry
Perhaps the future extraction consent should include one additional line:
“Your physiological readiness for surgery has been assessed.”
Because extraction safety should not depend on geography.
Whether a patient is treated in Mysore, Dublin, London, Tokyo, Dubai or Boston—
biology remains universal.
Perhaps the next revolution in oral surgery will not emerge from robotics, automation, or increasingly sophisticated instruments, but from something quieter and far more profound: a blood pressure cuff, a glucometer, a disciplined checklist, and the recognition that bleeding control does not begin after the tooth is removed but before local anesthesia is ever administered—for the safest extraction is rarely the fastest, but the one whose complications were anticipated, understood, and prevented before they ever had the opportunity to occur.

Author: Dr. Syed Nabeel
BDS, D.Orth, MFD RCS (Ireland), MFDS RCPS (Glasgow), MFDS RCS (Edinburgh)
Dr. Syed Nabeel is a clinician–scholar with over two decades of experience spanning orthodontics, neuromuscular dentistry, and digitally integrated diagnostics. As Clinical Director of Smile Maker Clinics Pvt. Ltd., he combines anatomical precision, occlusal science, and contemporary AI-enabled workflows in clinical care.
Founder of DentistryUnited.com (2004), he has built a professional community connecting over 40,000 dental professionals worldwide. He also founded Dental Follicle – The E-Journal of Dentistry (ISSN 2230-9489), an EBSCO-indexed peer-reviewed platform promoting interdisciplinary dental scholarship.
An educator, speaker, and advocate of collaborative learning, Dr. Nabeel continues to contribute through clinical practice, research, mentorship, and innovation—guided by the belief that knowledge creates greater value when shared.
Selected Scientific Reading
- Scottish Dental Clinical Effectiveness Programme (SDCEP). Management of Dental Patients Taking Anticoagulants or Antiplatelet Drugs.
- American Dental Association. Management of patients with bleeding risk during dental procedures.
- National Institute for Health and Care Excellence (NICE). Oral surgery and perioperative assessment guidance.
- Little JW et al. Dental Management of the Medically Compromised Patient.
- Malamed SF. Handbook of Local Anesthesia.
- Peterson LJ et al. Contemporary Oral and Maxillofacial Surgery.
- Lockhart PB et al. Dental management considerations in medically complex patients.
-
World Workshop on Oral Medicine consensus statements.