
Oral squamous cell carcinoma (OSCC) remains one of the most formidable challenges confronting oral healthcare professionals. Despite substantial advances in ablative surgery, reconstructive techniques, radiotherapy, systemic therapeutics, and precision oncology, improvements in long-term survival have been comparatively modest. This paradox reflects an enduring clinical reality: prognosis is determined far more by the stage at diagnosis than by therapeutic sophistication. Consequently, the greatest opportunity to reduce mortality lies not in expanding treatment options but in identifying malignant transformation before irreversible biological progression has occurred.
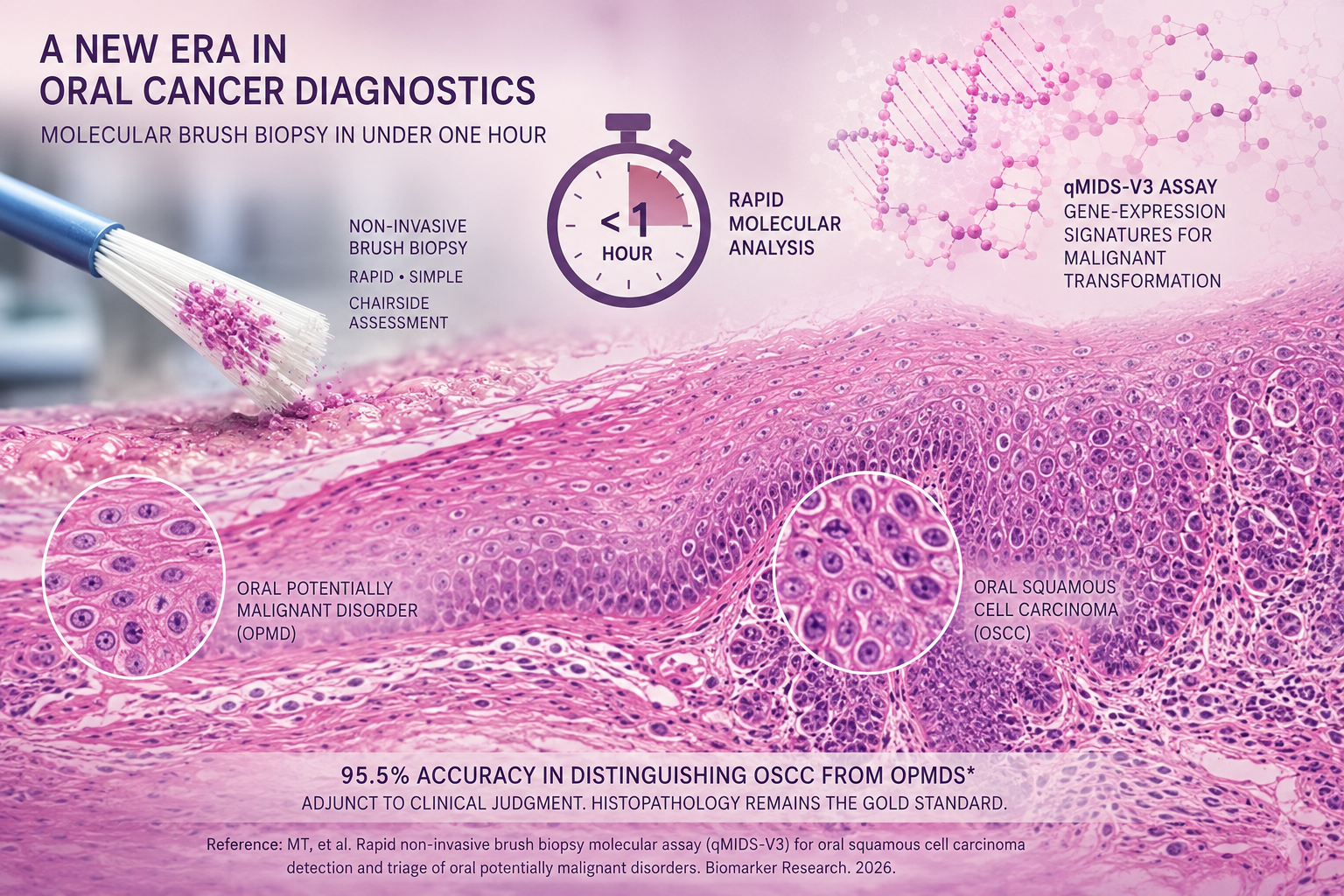
Against this backdrop, investigators from Queen Mary University of London have reported a noteworthy advance in molecular diagnostics that may reshape the early evaluation of oral potentially malignant disorders (OPMDs). Published in Biomarker Research (2026), their validation of the qMIDS-V3 molecular assay describes a rapid, non-invasive brush biopsy capable of distinguishing OSCC from OPMDs within approximately one hour. Analysing more than one thousand clinical specimens, the investigators reported an overall diagnostic accuracy of 95.5%, suggesting that molecular interrogation of exfoliated epithelial cells may substantially enhance contemporary approaches to oral cancer triage.
Unlike conventional exfoliative cytology, whose clinical utility has historically been constrained by variable sensitivity, operator dependence, and subjective cytomorphological interpretation, the qMIDS-V3 platform evaluates gene-expression signatures associated with malignant transformation. Rather than relying exclusively upon microscopic assessment of cellular morphology, the assay interrogates the molecular events that precede overt histological disruption. Such an approach reflects the broader evolution of oncology, in which biological behaviour increasingly complements morphology in disease classification and clinical decision-making.
For clinicians managing OPMDs, this distinction is particularly relevant. Daily practice frequently involves lesions whose biological potential cannot be predicted reliably by clinical appearance alone. Leukoplakia, erythroplakia, erythroleukoplakia, chronic non-healing ulceration, proliferative verrucous lesions, and selected lichenoid disorders continue to present diagnostic uncertainty despite careful examination. Current management often necessitates invasive biopsy, serial surveillance, or repeated histopathological assessment, even though a substantial proportion of lesions ultimately prove benign or demonstrate only low-grade dysplasia. Conversely, clinically innocuous lesions may harbour significant epithelial dysplasia or early invasive carcinoma, reinforcing the limitations of visual assessment alone.
A rapid molecular assay capable of objectively stratifying malignant risk before surgical intervention therefore represents a potentially important addition to contemporary diagnostic pathways. Rather than functioning as a replacement for biopsy, such technology may refine clinical prioritisation by identifying patients requiring urgent histopathological confirmation while permitting more rational surveillance strategies for lower-risk lesions. In this context, molecular brush biopsy should be viewed as a sophisticated adjunct to clinical judgement rather than a substitute for established diagnostic standards.
The implications extend beyond specialist oral medicine clinics. General dental practitioners remain the primary point of contact for patients with early mucosal pathology, yet differentiating reactive, inflammatory, traumatic, dysplastic, and malignant lesions remains one of the most demanding aspects of routine practice. A minimally invasive chairside molecular investigation performed during an initial consultation has the potential to reduce patient reluctance toward further investigation, facilitate earlier referral, and shorten the interval between first presentation and definitive diagnosis. Such benefits may prove particularly valuable in healthcare systems where access to specialist oral pathology services remains limited.
The potential relevance to countries such as India is especially compelling. With one of the highest global incidences of oral cancer, driven by extensive exposure to smokeless tobacco, areca nut, betel quid, cigarette smoking, alcohol consumption, and delayed clinical presentation, India continues to shoulder a disproportionate burden of disease. Population-based screening programmes have demonstrated clinical value but remain constrained by infrastructure, pathology capacity, workforce limitations, and economic considerations. A rapid molecular triage platform, if ultimately shown to be robust, affordable, and reproducible across diverse populations, could significantly strengthen community screening initiatives, outreach programmes, district hospitals, and primary oral healthcare services. Nevertheless, successful implementation would depend upon rigorous laboratory standardisation, external quality assurance, clinician training, regulatory oversight, and integration within established multidisciplinary cancer referral pathways.
Despite these promising findings, enthusiasm must remain tempered by scientific caution. Histopathological examination continues to represent the definitive diagnostic standard against which all emerging technologies must be judged. Brush biopsy evaluates only superficial epithelial cells and cannot provide essential architectural information upon which definitive diagnosis and treatment planning depend. Parameters including epithelial stratification, basement membrane integrity, stromal invasion, tumour thickness, depth of invasion, surgical margin status, perineural invasion, lymphovascular invasion, host stromal response, and tumour grading remain beyond the capability of exfoliative molecular analysis. These histopathological characteristics continue to underpin TNM staging, prognostic assessment, multidisciplinary treatment planning, and therapeutic decision-making. Consequently, no molecular assay can presently replace conventional tissue biopsy when invasive disease is suspected.
Equally important are the unanswered questions surrounding broader clinical implementation. Diagnostic performance requires prospective multicentre validation across geographically and ethnically diverse populations. Further evidence is needed to determine assay behaviour in inflammatory mucosal disorders, traumatic ulceration, oral lichen planus, candidal infections, post-radiotherapy mucosal alterations, recurrent disease, and surveillance following treatment for previous oral malignancy, where molecular signatures may potentially generate false-positive or clinically ambiguous findings. Parallel health economic analyses will also be essential to establish whether earlier detection and reductions in unnecessary biopsies justify the financial costs associated with widespread molecular testing.
The study also reflects a larger transformation occurring across diagnostic medicine. Pathology is progressively evolving from a discipline founded predominantly upon microscopic morphology to one integrating genomics, transcriptomics, molecular biomarkers, computational pathology, and artificial intelligence. Dentistry is increasingly participating in this transition. Future assessment of oral mucosal disease is likely to incorporate multimodal diagnostic platforms combining AI-assisted clinical imaging, quantitative salivary biomarkers, molecular brush cytology, genomic profiling, digital pathology, and predictive risk algorithms to identify malignant transformation at its earliest biological stages.
Viewed within this broader scientific landscape, the qMIDS-V3 assay represents one of the more clinically significant advances reported in oral oncology this year. Its greatest contribution lies not in challenging the primacy of histopathology, but in strengthening the diagnostic pathway that precedes it. Earlier biological recognition of malignant transformation may allow clinicians to intervene before architectural destruction, tissue invasion, and metastatic dissemination become established.
For practising dentists, oral physicians, oral and maxillofacial surgeons, and specialists in oral pathology, the clinical message remains unequivocal. Every persistent ulceration, unexplained erythroplastic or leukoplastic lesion, indurated mucosal abnormality, or suspicious alteration in the oral cavity warrants meticulous examination, comprehensive documentation, appropriate risk assessment, and timely tissue diagnosis where indicated. Molecular brush biopsy may soon become a valuable adjunct within this diagnostic continuum. Until large-scale validation studies, regulatory approval, and long-term outcome data firmly establish its clinical role, however, conventional histopathological examination remains the indispensable cornerstone of definitive diagnosis in oral oncology.
Reference
- MT, et al. Rapid non-invasive brush biopsy molecular assay (qMIDS-V3) for oral squamous cell carcinoma detection and triage of oral potentially malignant disorders. Biomarker Research. 2026.
- International Agency for Research on Cancer (IARC). GLOBOCAN Oral Cancer Statistics.
- World Health Organization. Oral Health Fact Sheet.

Author: Dr. Syed Nabeel
BDS, D.Orth, MFD RCS (Ireland), MFDS RCPS (Glasgow), MFDS RCS (Edinburgh)
Dr. Syed Nabeel is a clinician–scholar with over two decades of experience spanning orthodontics, neuromuscular dentistry, and digitally integrated diagnostics. As Clinical Director of Smile Maker Clinics Pvt. Ltd., he combines anatomical precision, occlusal science, and contemporary AI-enabled workflows in clinical care.
Founder of DentistryUnited.com (2004), he has built a professional community connecting over 40,000 dental professionals worldwide. He also founded Dental Follicle – The E-Journal of Dentistry (ISSN 2230-9489), an EBSCO-indexed peer-reviewed platform promoting interdisciplinary dental scholarship.
An educator, speaker, and advocate of collaborative learning, Dr. Nabeel continues to contribute through clinical practice, research, mentorship, and innovation—guided by the belief that knowledge creates greater value when shared.
In keeping with contemporary scholarly practice, Dr. Nabeel also embraces artificial intelligence as an editorial and research-support tool. AI may assist with literature synthesis, language refinement, and the organization of complex information; however, every article is conceived, critically evaluated, fact-checked, and editorially reviewed under his direct supervision. The opinions, interpretations, and final published content remain entirely his own, reflecting a commitment to scientific integrity, transparency, and evidence-based communication.