
Dr. Syed Nabeel
When I look back at articles I wrote for DentistryUnited in 2022 and 2023, I do not see obsolete ideas or outdated science. I see an earlier version of my own thinking. Those articles were carefully researched, firmly grounded in evidence, and written with the intention of helping clinicians navigate everyday practice. They explained procedures, compared materials, interpreted published studies, and translated scientific evidence into practical clinical guidance. They fulfilled precisely the purpose for which they were written.
Yet reading them today reveals something I had not anticipated. The most significant change over the past few years has not been in dentistry itself, nor in the pace at which scientific discoveries have emerged. It has been in the way I approach knowledge. Generative artificial intelligence has not simply altered the mechanics of writing; it has reshaped the intellectual process that precedes it.
That distinction matters.
My relationship with writing began long before large language models entered public consciousness. I have written continuously since the founding of DentistryUnited in 2004. During those two decades, successive website migrations, malware attacks, server failures, and changes in hosting providers erased a substantial part of that archive. Thousands of pages disappeared, taking with them years of clinical observations, editorials, and educational material. Although those losses remain deeply regrettable, enough of the surviving archive remains to document an unmistakable evolution—not merely in what I wrote, but in how I thought.
The earlier articles reflected the questions that defined much of contemporary dental practice. What does the current evidence recommend? Which material performs better? What protocol offers the most predictable outcome? How should a particular procedure be executed? These were appropriate questions in an era when accessing, organising, and synthesising scientific information demanded considerable effort. Knowledge itself was the limiting resource, and much of our intellectual energy was devoted to acquiring and organising it.
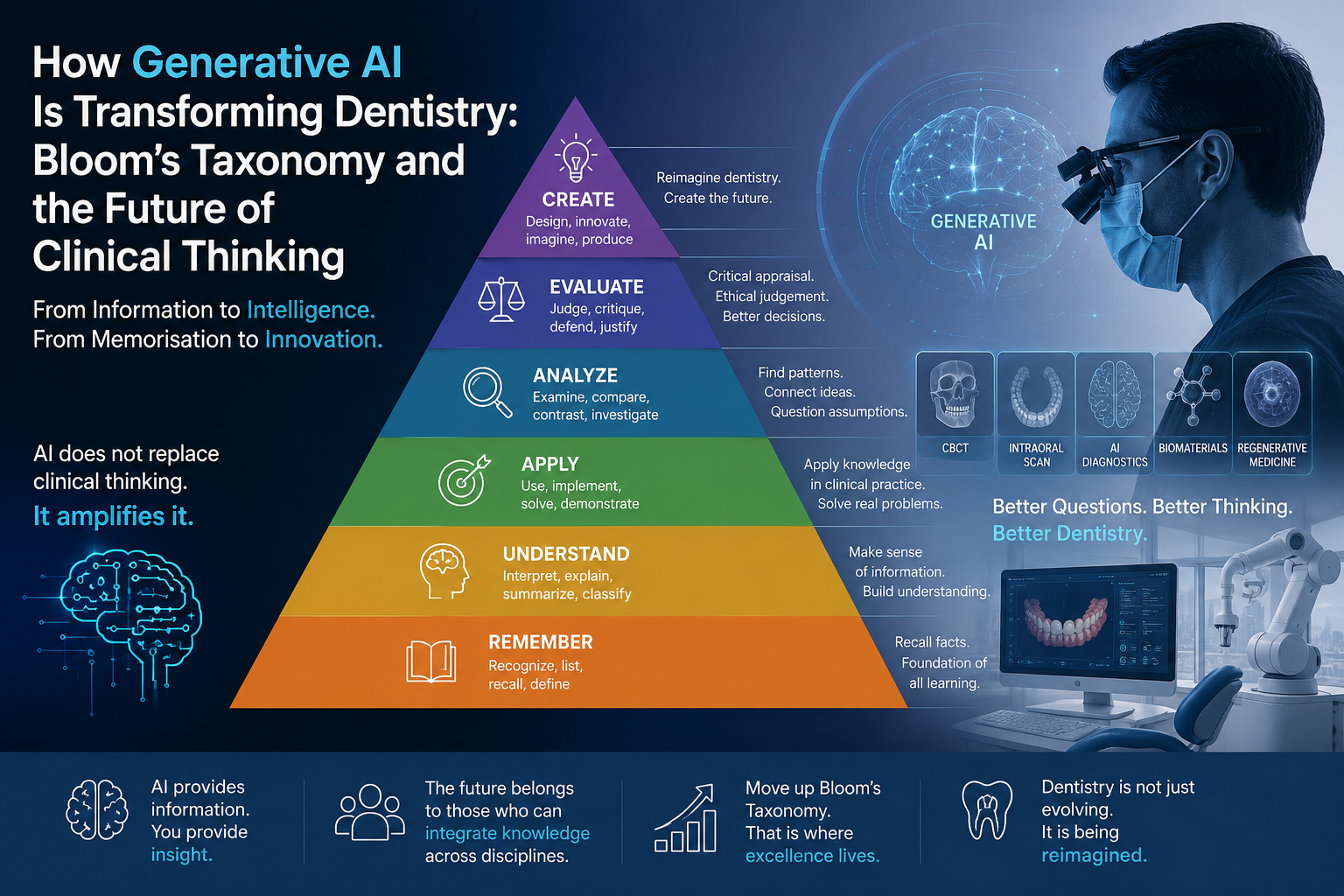
Educational psychologists recognised this long before the emergence of artificial intelligence. Bloom’s Taxonomy, first proposed in the 1950s, describes learning as a progression from remembering and understanding to application, analysis, evaluation, and ultimately creation. Dentistry has traditionally excelled at the lower and middle levels of this hierarchy. We memorised anatomy, mastered pathology, learnt clinical protocols, and applied them with increasing sophistication. That educational model produced generations of excellent clinicians because information was difficult to obtain and even more difficult to synthesise.
Generative AI changes that equation in a profound way. For the first time in modern professional history, access to information is no longer the principal constraint on intellectual work. Scientific papers can be located within seconds, competing viewpoints compared almost instantaneously, and vast bodies of literature synthesised in minutes rather than weeks. The consequence is not that expertise has become obsolete; rather, expertise is migrating upward. The competitive advantage of the clinician is moving away from information retrieval towards critical interpretation, interdisciplinary synthesis, ethical judgement, and creative problem solving.
This shift became apparent to me only when I began comparing my recent work with articles written just a few years earlier. The difference was not stylistic. It was cognitive. Earlier, my writing sought primarily to explain. Increasingly, it seeks to integrate. Rather than asking what a study concludes, I find myself asking how seemingly unrelated developments—artificial intelligence, regenerative biology, computational imaging, biomaterials, neuroscience, behavioural science, and systems engineering—might converge to reshape the future of dentistry. The questions have become broader, and in many respects, more important than the answers.
This is perhaps the greatest misconception surrounding artificial intelligence. Public discussion frequently frames AI as a substitute for human intelligence, encouraging understandable concerns about automation and professional displacement. My own experience has been almost the opposite. Artificial intelligence has functioned less as a replacement for thinking than as a catalyst for it. By reducing the cognitive burden associated with searching, organising, and summarising information, it has created more intellectual space for analysis, reflection, and imagination. The bottleneck is no longer information. It is the quality of the questions we choose to ask.
The implications extend well beyond writing. They reach into the foundations of dental education itself.
For more than a century, the structure of dental curricula has reflected an era in which information was scarce and difficult to access. Students were expected to memorise an ever-expanding body of anatomical detail, pathological classifications, pharmacological data, and procedural sequences because that knowledge could not be summoned instantly at the chairside. The educational model was entirely rational for its time. Mastery depended upon the ability to acquire, retain, and accurately reproduce information accumulated over years of study.
That educational philosophy now deserves thoughtful re-examination—not because knowledge has become less important, but because access to knowledge has been fundamentally transformed.
Artificial intelligence has not diminished the value of understanding anatomy, pathology, biomechanics, occlusion, or pharmacology. Quite the contrary. These disciplines remain the intellectual substrate upon which every clinical decision rests. What AI changes is the relative value of memorisation compared with interpretation. When factual information is available almost instantaneously, professional distinction increasingly resides in the ability to evaluate evidence critically, recognise its limitations, reconcile conflicting viewpoints, and apply knowledge judiciously to the unique circumstances of an individual patient.
Bloom’s Taxonomy anticipated this distinction decades before the first neural network was conceived. Remembering and understanding form the indispensable foundation of learning, but they were never intended to represent its culmination. The higher levels of cognition—analysis, evaluation, and creation—have always defined intellectual maturity. Generative AI has not rewritten Bloom’s hierarchy; it has simply accelerated our ascent through it. By reducing the cognitive effort devoted to retrieving information, it compels us to invest more energy in interpreting, questioning, integrating, and creating.
The implications for dentistry are profound.
A generation ago, a lecture describing the sequential stages of implant placement represented advanced education. Today, those procedural steps can be retrieved from multiple authoritative sources within seconds. Students can ask an AI assistant to explain each stage, compare competing implant systems, summarise systematic reviews, or generate visual illustrations of the procedure almost instantly. The educational value no longer lies in the recitation of established protocols. It lies in examining why those protocols exist, when they should be modified, and under what biological, systemic, or biomechanical circumstances conventional wisdom may no longer be appropriate.
The questions themselves have become more sophisticated.
How should implant planning change in a patient with poorly controlled diabetes, severe osteoporosis, or a history of bisphosphonate therapy?
How might artificial intelligence integrated with CBCT, intraoral scanning, facial analysis, and finite element modelling redefine prosthetically driven implant placement?
What role will regenerative biomaterials, tissue engineering, or personalised medicine play in reducing surgical morbidity over the next decade?
These are not questions that can be answered by memorising a textbook chapter. They require clinicians to synthesise knowledge from disciplines that have traditionally been taught in isolation. Increasingly, dentistry intersects with computer science, biomedical engineering, molecular biology, behavioural psychology, health economics, ethics, and data science. The modern clinician must become not merely a consumer of information but an integrator of ideas.
This, perhaps, represents the most significant intellectual consequence of generative AI. It dissolves many of the practical barriers that once separated disciplines. Scientific literature from medicine, engineering, neuroscience, materials science, epidemiology, economics, and public health can now be explored within a single intellectual conversation. Connections that once required months of literature review can emerge during the course of an afternoon’s inquiry. The technology itself does not create insight, but it dramatically enlarges the landscape within which insight can occur.
Looking back, I recognise that my earlier articles were largely concerned with explanation. They attempted to clarify evidence, simplify complexity, and make contemporary knowledge accessible to practising clinicians. That objective remains valuable and will always remain an essential function of professional writing.
Yet my more recent work has gradually shifted towards a different ambition.
Rather than asking what is known, I increasingly ask what existing knowledge makes possible.
Rather than examining discoveries in isolation, I find myself exploring the convergence of technologies that are developing simultaneously but are too often discussed independently. Artificial intelligence, digital dentistry, robotics, advanced imaging, regenerative biology, genomics, precision medicine, and computational diagnostics are not separate revolutions. They are interacting systems whose combined impact will almost certainly exceed the influence of any individual technology.
This shift—from explanation towards synthesis—is, in my view, the defining intellectual opportunity presented by artificial intelligence.
Importantly, this evolution should not be mistaken for technological determinism. AI does not absolve clinicians of the responsibility to think critically. On the contrary, it demands greater intellectual discipline. Large language models are capable of remarkable synthesis, but they are also capable of confident error, misplaced certainty, incomplete reasoning, and subtle factual distortion. Scientific scepticism therefore becomes more important, not less. The clinician must remain the final arbiter of evidence, weighing biological plausibility, methodological quality, clinical experience, and patient values before accepting any recommendation, whether generated by an algorithm or published in a prestigious journal.
This may prove to be one of the great paradoxes of the AI era. As machines become increasingly capable of processing information, the distinctly human qualities of judgement, curiosity, ethical reasoning, empathy, and imagination become even more valuable. These are not competencies that artificial intelligence replaces. They are precisely the competencies that determine whether artificial intelligence is used wisely.
For dentistry, the implications extend beyond clinical practice into research itself. AI is already accelerating hypothesis generation, assisting systematic reviews, identifying patterns within large datasets, modelling disease progression, and supporting personalised treatment planning. The pace of discovery is likely to increase substantially over the coming decade. Yet the most transformative questions will continue to originate not from algorithms but from investigators capable of recognising problems that have not yet been articulated.
When I revisit my own writing from previous years, I therefore see continuity rather than contradiction. Those articles reflected the best understanding I possessed at that point in my professional journey. They were necessary steps in an intellectual progression that continues today. Artificial intelligence did not replace that journey; it expanded its horizon.
Every technological revolution changes the tools of a profession. Only a few change the way its practitioners think.
Generative AI belongs to the latter category.
Its greatest contribution to dentistry may ultimately prove not to be faster documentation, automated workflows, or accelerated literature reviews. It may be that it encourages clinicians, educators, and researchers to move beyond the acquisition of knowledge towards its integration; beyond technical competence towards intellectual adaptability; and beyond answering established questions towards asking better ones.
The future of dentistry will not belong simply to those who know the most.
Knowledge is becoming increasingly ubiquitous.
Wisdom remains scarce.
The profession will increasingly be shaped by clinicians who can combine scientific evidence with critical judgement, integrate insights across disciplines, question accepted assumptions with intellectual humility, and employ artificial intelligence not as a substitute for thought, but as an instrument that expands the reach of human imagination.
In that sense, the most important innovation of the AI era may not be artificial intelligence itself.
It may be the rediscovery of what constitutes exceptional human intelligence.

About the Author
Dr. Syed Nabeel is a clinician-scholar, educator, and founder of DentistryUnited.com, a global knowledge platform established in 2004 to promote evidence-based dentistry, interdisciplinary learning, and professional collaboration. Over more than two decades of clinical practice spanning orthodontics, neuromuscular dentistry, digital workflows, and practice innovation, his professional interests have progressively expanded towards the intersection of artificial intelligence, cognitive science, education, and the future of healthcare.
In recent years, his writing has explored how generative AI, machine learning, computational diagnostics, digital dentistry, systems thinking, and regenerative medicine are reshaping not only clinical workflows but the very nature of clinical reasoning. Rather than viewing artificial intelligence as a replacement for professional judgement, he advocates its responsible use as an intellectual partner that augments evidence synthesis, stimulates interdisciplinary thinking, and supports lifelong learning while preserving the primacy of human ethics, empathy, and clinical decision-making.
Dr. Nabeel is the Founder and Editor-in-Chief of Dental Follicle – The E-Journal of Dentistry (ISSN 2230-9489), a peer-reviewed publication dedicated to advancing contemporary dental scholarship. His recent work has focused on the evolving relationship between artificial intelligence, dental education, precision diagnostics, curriculum reform, and the future of clinical practice, reflecting a broader interest in how emerging technologies are redefining the way dentists think, learn, and innovate.