
Can Dental Robots Prepare Crowns? A Critical Review of the University of Basel Intraoral Robot : An investigative review of the University of Basel miniature dental robot
A report published on 25 June 2026 has drawn attention to a miniature intraoral robot being developed to prepare teeth for crowns1. The concept is compelling: scan the patient, digitally plan the preparation, attach a custom splint, allow a small robot to execute the planned reduction, and potentially deliver the definitive restoration without asking the patient to return for another preparation appointment.
For restorative dentists, this is not merely another “AI in dentistry” headline. Crown preparation is one of the most technique-sensitive procedures in daily practice. It requires controlled reduction, appropriate taper, a readable margin, preservation of sound tooth structure, management of soft tissues, and continuous clinical judgement. A device that can reliably assist with even part of that sequence could affect clinical workflow, laboratory communication, training and patient expectations.
But the important word is could.
The University of Basel system is an early-stage engineering development, not a commercially deployable clinical robot. Its reported results are encouraging, yet they should be interpreted carefully before claims of “one-visit automated crowns” become part of everyday dental marketing.
What has actually been developed?
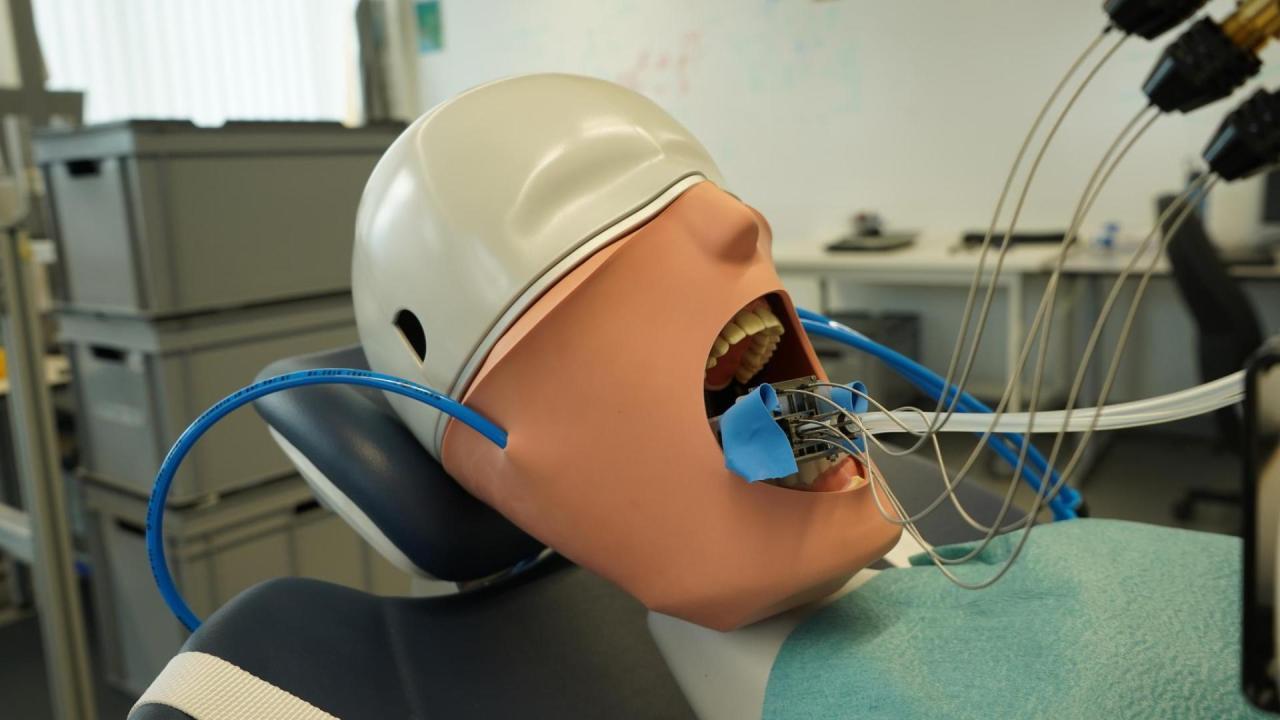
The device is a small intraoral robot, approximately the size of a cork, connected to external controls by flexible cables. It is intended to be fixed to a patient-specific splint fabricated from a digital scan. This splint is central to the concept: rather than attempting to track a freely moving patient from outside the mouth, the robot is mechanically coupled to the dentition and should therefore move with the patient’s head.
The proposed workflow is straightforward in theory:
1. A diagnostic intraoral scan is taken.
2. The clinician digitally plans the crown preparation.
3. A customised splint is designed and fabricated.
4. The robot is mounted on the splint.
5. A larger bur performs occlusal reduction.
6. A finer bur performs axial reduction.
7. The crown can be designed or ordered from the same digital dataset.
The reported positional error was below 0.2 mm in testing. Drilling forces were reported to remain below five newtons. However, the tests were conducted on synthetic resin models and ceramic material designed to approximate enamel hardness—not on living teeth in a clinical setting. (Dentistry.co.uk)
Why crown preparation is an attractive target for robotics
Crown preparation is repetitive, measurable and increasingly digital. Unlike many dental procedures, it can be represented as a planned three-dimensional reduction envelope. CAD software can define the desired preparation, minimum material thickness, occlusal clearance, taper and finish-line geometry.
This makes it suitable for robotic assistance.
A robot does not become fatigued, does not lose concentration late in a long clinical day, and can theoretically follow a pre-defined path with consistency. In principle, robotic preparation could reduce variability in reduction depth and help avoid under-reduction, which compromises material thickness, or over-reduction, which sacrifices valuable tooth structure.
The appeal is especially strong in a digital same-day workflow. If the preparation can be planned accurately before cutting begins, the restoration can potentially be designed in parallel. That could shorten chair time and reduce the traditional sequence of preparation, previsualization, laboratory turnaround and final cementation.
Yet crown preparation is not simply a geometric task. It is a biological and clinical task. The challenge for any robot is not merely cutting a shape; it is responding safely when the mouth does not behave like a digital model.
The central question: can a robot manage the clinical realities?
The most significant limitation of the Basel prototype is that it has not yet demonstrated performance in patients.
A laboratory model does not bleed, salivate, gag, move unpredictably, present a subgingival carious margin, have a cracked cusp, or reveal a pulp horn closer than expected. It does not have restricted opening, a prominent tongue, anxious behaviour, a mobile tooth, periodontal inflammation or an opposing dentition that changes the practical design of the restoration.
A clinician preparing a tooth continuously adjusts the plan. The dentist may decide that a cusp needs protection, that a margin must be moved, that a ferrule is inadequate, that a build-up is required, or that the tooth is no longer a suitable crown candidate. These decisions occur before and during preparation.
For this reason, the most realistic near-term role for such technology is likely to be robot-assisted preparation under direct dentist supervision, rather than autonomous dentistry.
Accuracy: impressive figures, but context matters
The reported positional error of less than 0.2 mm is promising for a miniature device operating within the mouth. However, accuracy must be assessed in relation to the clinical endpoint.
A discrepancy of 0.2 mm may be acceptable in broad occlusal reduction, but it can be highly relevant at a finish line, near an adjacent tooth, or in a thin remaining dentine zone. In crown preparation, precision is not only about reaching a planned surface. It is also about preserving biologically safe margins, avoiding iatrogenic damage, controlling convergence and ensuring that the final preparation is readable by the scanner, technician and restorative material selected.
Other robotic crown-preparation research has reported substantially higher precision under controlled conditions. A 2025 first-in-human study of a semi-automated robotic tooth-preparation system reported a root mean square deviation of 39 micrometers from the planned preparation in six completed cases, with no reported adverse events. That study is important because it moves beyond bench testing—but it was still small, highly controlled and does not establish broad clinical equivalence or superiority. (PMC)
Similarly, laboratory research on automated robotic crown preparation has suggested improved accuracy and shorter operating times compared with guide-based approaches. Such findings support the direction of travel, but they do not eliminate the need for larger independent clinical trials. (PubMed)
The safety issue is more important than the speed issue
Public discussion often focuses on whether robots can prepare teeth faster than dentists. That is not the key question.
The key question is whether the system can stop safely and predictably when something unexpected happens.
The Basel researchers are working towards integrating positional sensors, including the ability to maintain knowledge of its location after an interruption such as a power failure. That is a sensible engineering priority. A dental robot needs reliable fail-safe mechanisms, real-time tracking, force monitoring, emergency stop protocols and clear clinician override at every stage. (Dentistry.co.uk)
In a live clinical setting, the system would also need to account for:
* patient movement and sudden jaw closure;
* splint displacement or incomplete seating;
* bur wear, clogging or fracture;
* saliva, blood and reduced visibility;
* variation in enamel, dentine, restorative materials and caries;
* heat generation and pulpal protection;
* soft-tissue proximity;
* adjacent-tooth injury;
* inaccurate scans or planning errors;
* unexpected tooth fractures or inadequate retention.
A robot may execute a flawed plan very consistently. Therefore, the quality of the scan, diagnosis, preparation design and dentist oversight may matter as much as the mechanics of the robot itself.
Does this mean fewer appointments?
Possibly—but not automatically.
The headline promise is that the robot may enable crown preparation and restoration delivery in a single visit. That claim depends on several conditions being met:
* the tooth must be appropriately diagnosed and treatment-planned in advance;
* the scan must be accurate;
* the splint must fit precisely;
* the preparation must proceed without complication;
* the definitive crown must be designed, milled or printed quickly;
* occlusion, contacts, shade and characterization must be managed within the same visit;
* no endodontic, periodontal or restorative complication should arise.
For selected posterior cases with straightforward indications, a same-day workflow may be realistic. For heavily broken-down teeth, deep margins, complex occlusion, aesthetic anterior restorations, multi-unit work or cases requiring staged treatment, robotics is unlikely to remove the need for clinical judgement, temporization or additional visits.
The technology may reduce appointments in selected cases. It should not yet be presented as a universal replacement for conventional crown workflows.
What this could mean for dentists
The most likely impact is not that dentists will become redundant. Instead, the dentist’s role may shift further upstream and downstream.
Before preparation, the dentist will need to diagnose, decide indication, determine restoration type, assess periodontal and endodontic status, establish margin design and approve the digital plan.
During preparation, the dentist may supervise the robot, manage isolation, verify safety, intervene when required and make real-time clinical decisions.
After preparation, the dentist remains responsible for evaluating fit, occlusion, aesthetics, cementation or bonding, patient comfort and long-term review.
In other words, the robot may eventually automate a constrained mechanical component of treatment. It does not automate diagnosis, ethics, consent, complication management or responsibility.
Regulatory and medico-legal questions
Before clinical adoption, this technology will need to satisfy far more than engineering performance.
It will require evidence of safety and effectiveness through clinical trials, regulatory clearance as a medical device, robust cybersecurity, documented maintenance standards, operator training and clear liability frameworks.
If a robot removes excessive tooth structure, damages an adjacent tooth or follows an incorrect digital plan, where does responsibility lie? The clinician who approved the plan? The practice? The manufacturer? The software provider? The technician who designed the crown? The answer will vary by jurisdiction, but the dentist is unlikely to be removed from the chain of accountability.
In India, any future adoption would also need to align with applicable medical-device regulation, professional standards, informed-consent requirements and local practice infrastructure. A clinic purchasing such a system would need to consider not only capital cost but also service support, consumables, training, calibration, software updates and insurance implications.
The wider context: dentistry is already becoming robotic
Dental robotics is not a completely new idea. Robot-assisted implant surgery has already demonstrated that computer-guided systems can improve positional control in selected surgical workflows. Research is also progressing in robotic endodontics, prosthodontics and automated crown design.
What is new about the Basel concept is its compact intraoral format and its attempt to place the robotic mechanism directly inside the patient’s mouth. That is both its innovation and its engineering challenge.
Earlier automated tooth-preparation work has included laser-based systems and robotic approaches using digital planning. The field has been developing for at least a decade, but the path from proof-of-concept to routine clinical use is long. (Nature)
Verdict: promising prototype, not yet a clinical revolution
The miniature intraoral robot from the University of Basel is a credible and interesting development. It addresses a genuine problem in restorative dentistry: how to deliver more consistent tooth preparation while integrating digital scanning, planning and restoration manufacture.
Its strongest feature is the patient-specific splint-based design, which may offer a practical way to compensate for head movement. Its most important unanswered questions are clinical safety, performance in real mouths, margin quality, management of unexpected findings, patient comfort, workflow time, cost and regulatory approval.
For now, the appropriate conclusion is neither dismissal nor hype.
This is not yet a robot dentist replacing the clinician. It is an early prototype pointing towards a future in which carefully supervised robotic systems may help dentists perform selected crown preparations with greater consistency and potentially fewer appointments.
The profession should welcome the research—but demand rigorous clinical evidence before allowing a machine to cut living tooth structure.
DentistryUnited will continue to follow developments in dental robotics, digital prosthodontics and AI-assisted clinical workflows.
Further Reading:
- https://www.unibas.ch/en/News-Events/News/Uni-Research/A-mini-robot-to-simplify-dental-treatment.html
- Miniature Intraoral Robot (MIR) for Minimally Invasive Tooth Preparation
IEEE Transactions on Medical Robotics and Bionics (2026), doi: 10.1109/TMRB.2026.3682629